
GLP-1 treatment produces measurable improvements in metabolic health markers that go well beyond weight loss alone, with implications for long-term cardiovascular and metabolic risk.
Most people who start a GLP-1 weight loss programme are focused on the number on the scale. Understandably so. But the clinical outcomes data from supervised programmes tell a more interesting story: the metabolic improvements that come alongside weight loss are, in many cases, as significant as the weight loss itself.
Cholesterol profiles normalise. Blood pressure drops. Pre-diabetes reverses. These are not minor secondary benefits. In a population where obesity is associated with over 50 weight-related conditions, the ability of GLP-1 medications like Wegovy (semaglutide) and Mounjaro (tirzepatide) to improve multiple metabolic risk markers simultaneously is what moves them from weight loss treatments into the territory of preventative metabolic medicine.
This article explains what happens to cholesterol, blood pressure, and blood sugar during GLP-1 treatment, why it happens, and what the real-world data from supervised programmes shows.
Why weight loss alone does not explain all the metabolic benefits
The intuitive explanation for the metabolic improvements seen with GLP-1 treatment is simple: people lose a significant amount of weight, and weight loss improves metabolic markers. That is true. But it is not the complete picture.
A 2025 analysis of results from the SELECT trial, published following the landmark cardiovascular outcomes study of Wegovy, found that semaglutide reduced cardiovascular risk regardless of how much weight participants lost. Patients who lost minimal weight still showed meaningful reductions in the risk of heart attack and stroke. Researchers attributed this to direct biological effects of the medication: reduced inflammation, improved blood pressure regulation, and direct effects on blood vessel walls that were independent of the weight change.
This has important clinical implications. It means GLP-1 medications are not simply tools that work by making people lighter. They are pharmacological agents with direct cardiometabolic mechanisms, and the combination of those direct effects with the secondary benefits of significant weight loss is what produces the outcome profile seen in supervised programme data.
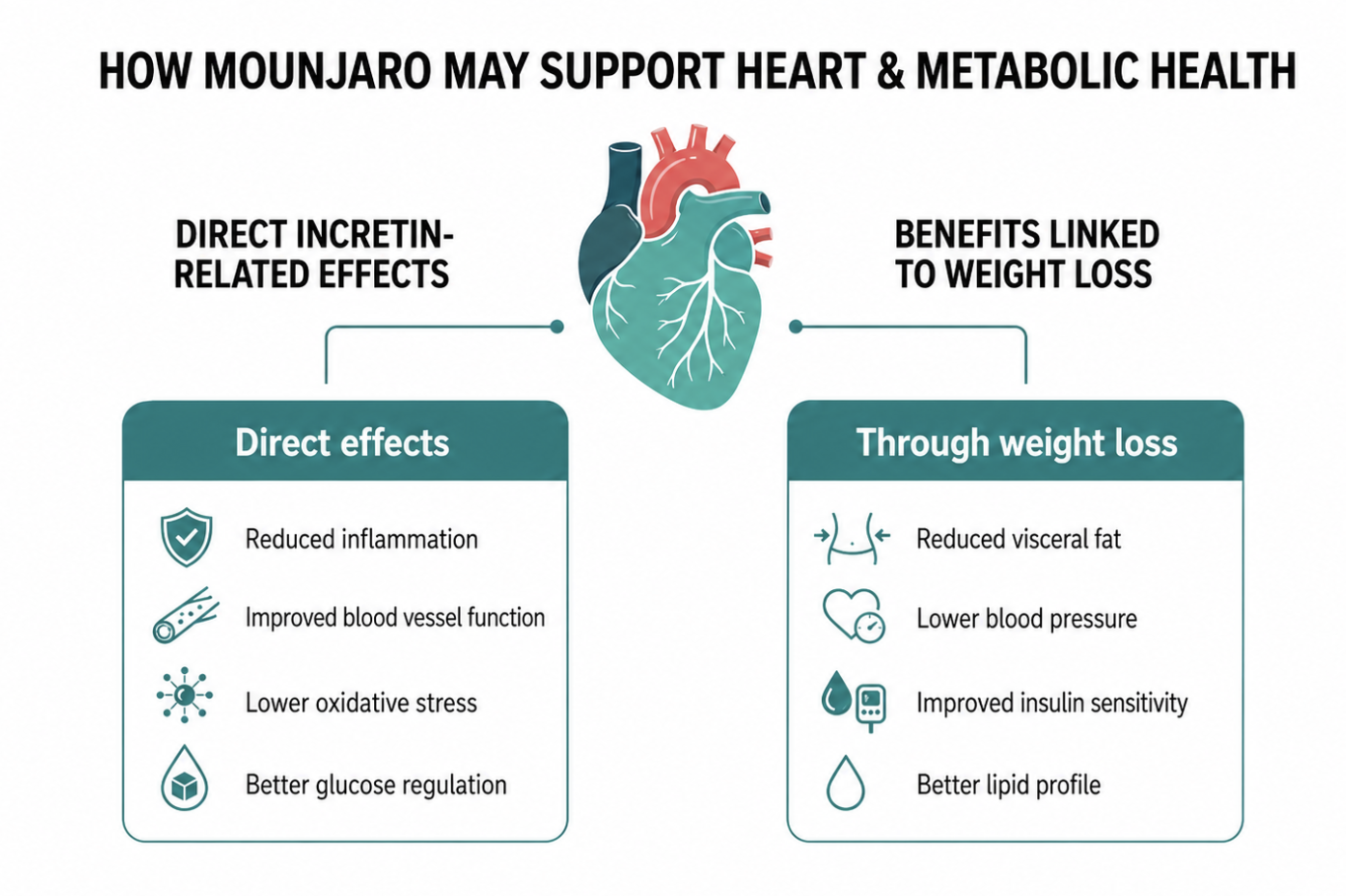
GLP-1 medications act through two parallel channels: direct effects on blood vessels, inflammation, and glucose regulation, and secondary effects through weight loss itself.
HbA1c: what it measures and why reversal matters
Understanding the HbA1c test
HbA1c (glycated haemoglobin) is a blood test that measures the average blood glucose level over the previous three months. When blood sugar is consistently elevated, glucose binds to haemoglobin molecules in red blood cells, forming glycated haemoglobin. The higher the proportion of glycated haemoglobin, the higher the average blood sugar over that period.
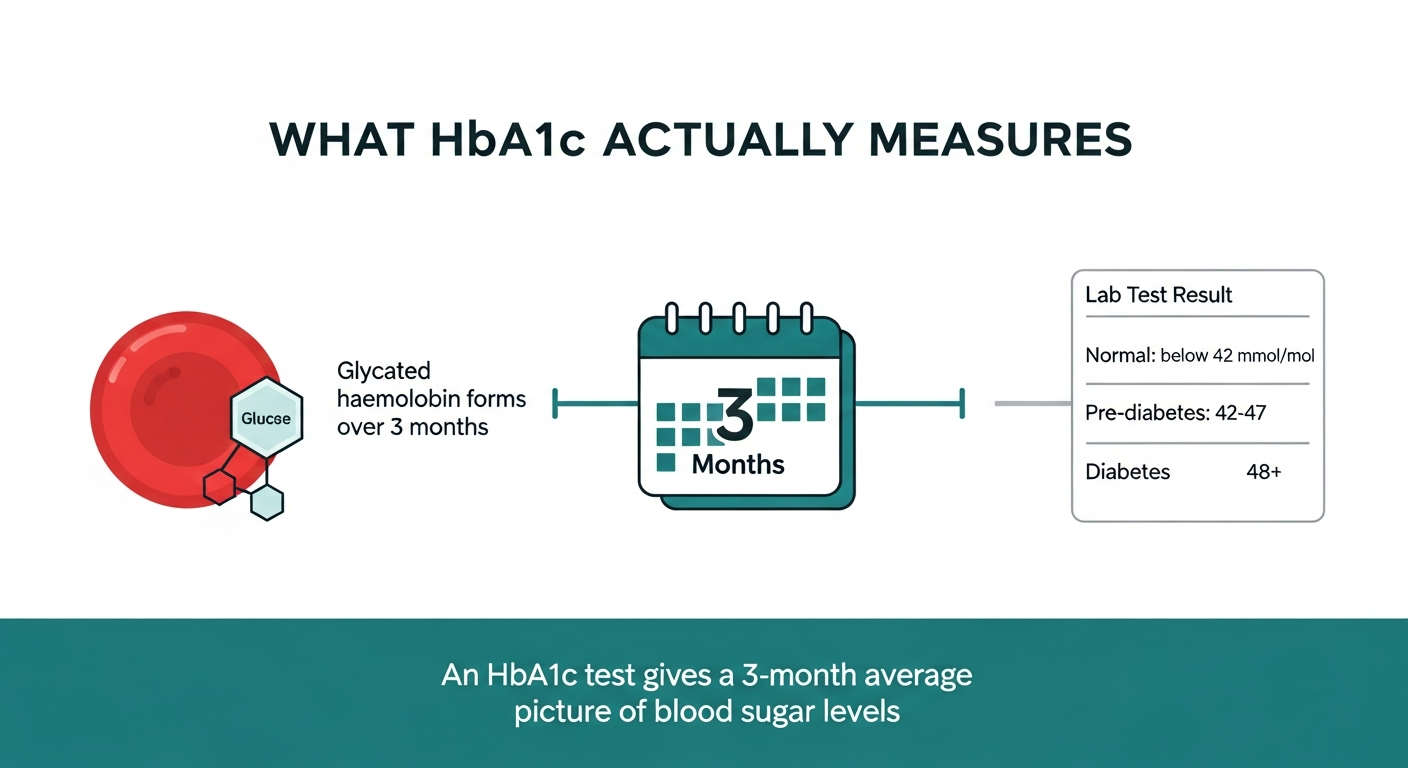
HbA1c measures the average blood sugar level over three months by tracking how much glucose has attached to haemoglobin. Pre-diabetes is defined as 42 to 47 mmol/mol. Above 48 indicates type 2 diabetes.
The UK reference ranges are: below 42 mmol/mol is normal; 42 to 47 mmol/mol indicates pre-diabetes; 48 mmol/mol or above indicates type 2 diabetes. Pre-diabetes is not a guaranteed path to diabetes, but it is a significant risk marker. Approximately 5 to 10% of people with pre-diabetes develop type 2 diabetes every year, and the cardiovascular risk associated with elevated blood sugar begins at pre-diabetic levels, not just at the diabetes threshold.
What the outcome data shows
In a large retrospective cohort study of over 23,000 adults on semaglutide, published in JAMA Internal Medicine in 2025, semaglutide initiation was associated with significant reductions in HbA1c at 13 to 24 months. Participants with pre-diabetes at baseline showed substantially higher rates of returning to normal blood sugar compared to those on placebo.
The Novo Nordisk OASIS 4 trial data presented at ObesityWeek 2025 found that 71.1% of participants with pre-diabetes achieved normal blood glucose by week 64 on semaglutide, compared to 33.3% on placebo.
In supervised programme data from Voy, published in Diabetes Obesity and Metabolism in 2025, 100% of pre-diabetic members achieved complete HbA1c reversal during treatment. For readers considering Wegovy, Voy outlines the clinician-reviewed treatment process, including assessment, dosing, delivery, and ongoing support.
|
“ |
100% of pre-diabetic members in a supervised Wegovy programme achieved complete HbA1c reversal. In the OASIS 4 trial, 71.1% of pre-diabetic participants reached normal blood glucose at week 64 on semaglutide versus 33.3% on placebo. Voy outcome data published in Diabetes Obesity and Metabolism, 2025. OASIS 4, ObesityWeek 2025. Individual results may vary. Treatment subject to clinical suitability. |
Why the mechanism produces this outcome
GLP-1 receptor activation directly improves glycaemic control through three parallel mechanisms. First, it stimulates insulin secretion from the pancreas in response to meals, but only when blood glucose is elevated. This glucose-dependent action means it lowers blood sugar without the hypoglycaemia risk associated with insulin or sulphonylureas. Second, it suppresses glucagon, the hormone that prompts the liver to release stored glucose into the bloodstream. Third, it slows gastric emptying, which reduces the speed at which dietary carbohydrates enter the bloodstream and blunts the post-meal glucose spike.
Together, these mechanisms significantly reduce the chronic low-level glucose elevation that defines pre-diabetes. When combined with the reduction in visceral fat that accompanies significant weight loss, which itself improves insulin sensitivity, the result is a sustained improvement in glycaemic control that in many cases returns HbA1c to normal range.
Cholesterol: the lipid profile improvements
What changes and why
GLP-1 treatment consistently improves multiple components of the lipid profile. Across clinical trial and real-world data: LDL cholesterol falls, triglycerides fall, and HDL cholesterol rises. The combination of these changes represents a meaningful reduction in cardiovascular risk.
The mechanism operates through two channels. Direct GLP-1 receptor activation reduces hepatic lipogenesis, the process by which the liver produces triglycerides from excess carbohydrate and fat. It also appears to reduce inflammation in atherosclerotic plaques and improve endothelial function, the health of the cells lining blood vessel walls. These effects are partially independent of weight loss.
The secondary pathway is the weight loss itself. Visceral fat is metabolically active tissue that secretes free fatty acids into the portal circulation, driving elevated triglycerides and LDL. When visceral fat deposits reduce significantly, lipid production falls accordingly.
What the data shows
In the SELECT trial, which followed over 17,000 people for a mean of 40 months, semaglutide produced significant reductions in LDL cholesterol, triglycerides, and high-sensitivity C-reactive protein (a marker of cardiovascular inflammation), alongside the 20% reduction in major adverse cardiovascular events.
In the SCOPE real-world study of over 4,400 adults on Wegovy for 52 weeks, published in 2025, lipid panel improvements were documented alongside weight loss. HDL increased by approximately 4% on semaglutide. In SURMOUNT-5, tirzepatide showed HDL increases of 7 to 8% versus 4% with semaglutide, reflecting its additional GIP receptor mechanism.
In supervised Voy programme data published in Diabetes Obesity and Metabolism in 2025, 72% of members showed improved cholesterol levels, with over 30% achieving full normalisation of lipid profiles. These outcomes reflect the combined effect of GLP-1 pharmacology and the sustained significant weight loss that comes from a properly supervised and monitored programme.
|
“ |
72% of supervised programme members improved cholesterol levels on Wegovy. More than 30% achieved full lipid profile normalisation. In the SELECT trial, semaglutide reduced LDL, triglycerides, and inflammatory markers alongside a 20% reduction in major cardiovascular events. Voy outcome data, Diabetes Obesity and Metabolism, 2025. SELECT trial, NEJM, 2023. Individual results may vary. |
Blood pressure: the cardiovascular case for treating weight medically
Why obesity drives high blood pressure
Hypertension and obesity are deeply interconnected. Excess weight increases blood volume, raises cardiac output, activates the renin-angiotensin-aldosterone system (which raises blood pressure through sodium retention and vasoconstriction), and drives sympathetic nervous system overactivity. Visceral fat in particular is a metabolically active source of angiotensinogen, a precursor to angiotensin II, which directly causes blood vessel constriction.
Treating weight medically, therefore, addresses blood pressure through multiple mechanisms: reduced blood volume, lower cardiac demands, suppressed renin-angiotensin activation, and reduced visceral fat mass.
Direct GLP-1 effects on blood pressure
GLP-1 receptor activation has direct vasodilatory effects independent of weight change. GLP-1 receptors are present in blood vessel walls and in the kidney, where GLP-1 activation promotes natriuresis, the excretion of sodium, which lowers blood volume and therefore blood pressure. GLP-1 also reduces the production of atrial natriuretic peptide (ANP), which has a vasodilatory effect.
The 2025 ScienceDaily analysis of the SELECT trial confirmed that blood pressure reduction was not solely weight-dependent: semaglutide improved blood pressure regulation through direct effects on the vasculature, independent of the degree of weight loss achieved.
What the outcome data shows
In the SCOPE real-world study of Wegovy, systolic blood pressure fell significantly at 52 weeks alongside weight loss. In SURMOUNT-5, tirzepatide showed greater blood pressure reduction than semaglutide: the absolute reduction in systolic blood pressure was larger with tirzepatide, reflecting its additional GIP receptor mechanism and greater weight loss.
In supervised Voy programme data published in Cureus in 2025, members on GLP-1 treatment achieved a 6.5% reduction in systolic blood pressure. Combined with the cholesterol and HbA1c improvements from the same programme, the cardiometabolic picture is one of sustained, broad metabolic improvement rather than isolated weight loss.
|
“ |
Supervised Voy programme members achieved a 6.5% reduction in systolic blood pressure during GLP-1 treatment. Semaglutide reduced blood pressure through both weight-dependent and direct vascular mechanisms, confirmed in SELECT trial analysis, 2025. Voy outcome data published in Cureus, 2025. ScienceDaily analysis of SELECT trial, 2025. Individual results may vary. |
The three metabolic markers most significantly improved by GLP-1 treatment: HbA1c, cholesterol, and blood pressure. All are monitored in supervised programmes and documented in peer-reviewed publications.
Why supervised monitoring changes what is achievable
The gap between clinical trial outcomes and real-world programme outcomes is not just about the medication. In Voy’s published JMIR data (2025), supervised programme members achieved 24% average weight loss at 12 months versus 16% in clinical trials. The metabolic improvements are similarly elevated in supervised settings.
The reasons are straightforward. Supervised programmes monitor HbA1c, lipid profiles, and blood pressure at baseline and throughout treatment, which means changes are caught early and can be fed back into clinical decisions. Dose adjustments can be made based on metabolic response as well as weight loss. And adherence, the foundational requirement for any of these outcomes, is significantly better in supervised programmes with active support: Voy’s programme achieved 35% better treatment retention than the industry benchmark.
For people with pre-diabetes, hypertension, or elevated cholesterol who are also living with excess weight, this combination of outcomes is the case for treating weight as a medical priority. The evidence increasingly supports positioning GLP-1 treatment not as obesity medication but as preventative metabolic care.
Frequently asked questions
How quickly does Wegovy improve HbA1c?
HbA1c improvements begin within the first few months of treatment as blood sugar control improves through GLP-1 receptor mechanisms. Because HbA1c reflects the average blood glucose over three months, a meaningful change in the test result typically becomes visible at the three-month mark and continues to improve as weight loss compounds. Complete reversal of pre-diabetes has been documented in supervised programme data by 12 months.
Does Wegovy lower cholesterol directly or just through weight loss?
Both. GLP-1 receptor activation has direct effects on hepatic lipid production and on endothelial function that are partially independent of weight change. However, the most significant lipid improvements are associated with sustained significant weight loss, which reduces visceral fat and the free fatty acid load on the liver. The two mechanisms work together and their combined effect in supervised programmes with 20%+ weight loss is more pronounced than either alone.
How much does blood pressure fall on GLP-1 treatment?
Published data from supervised Wegovy programmes shows a 6.5% reduction in systolic blood pressure. In large real-world studies like SCOPE, systolic blood pressure reduction was documented at both 52 and 68 weeks. The magnitude of reduction depends on starting blood pressure, degree of weight loss, and individual response. Direct vascular effects of GLP-1 contribute beyond weight loss alone, as confirmed in SELECT trial analysis.
Are these metabolic improvements maintained after stopping treatment?
Published evidence consistently shows that HbA1c, cholesterol, and blood pressure improvements regress when GLP-1 treatment is discontinued, in parallel with the weight regain that typically follows cessation. ICER’s 2025 review of semaglutide and tirzepatide confirmed this pattern. This is consistent with GLP-1 medications being chronic condition treatments rather than curative interventions. The metabolic improvements are maintained with continued supervised treatment.
What metabolic monitoring should be included in a supervised programme?
A properly supervised GLP-1 programme should monitor HbA1c, full lipid panel, blood pressure, weight, and renal function at baseline and at regular intervals during treatment. This allows the clinical team to track metabolic response alongside weight loss, adjust dosing if needed, and identify any markers that are not improving as expected. Voy’s supervised Wegovy programme includes this monitoring as part of its standard clinical model.
Is Wegovy approved specifically for cardiovascular protection?
Yes. Following the SELECT trial, Wegovy received FDA approval in the United States and is indicated in the UK not just for weight management but for reducing the risk of major adverse cardiovascular events in adults with established cardiovascular disease and obesity or overweight. This makes it the first and currently only anti-obesity medication with a dedicated cardiovascular outcomes indication. Tirzepatide (Mounjaro) does not yet have equivalent dedicated cardiovascular outcomes evidence, though data from ongoing trials is expected.
|
This article is for informational purposes only and does not constitute medical advice. Always consult a healthcare professional before starting any weight loss treatment. Individual results may vary. Treatment is subject to clinical suitability. Results achieved alongside a reduced-calorie diet and increased physical activity. |

